Help first responders find important information quickly in an emergency.
A simple medical form and magnetic packet for your refrigerator — one of the first places responders check.
How It Works
Three quick steps to make sure your critical information is ready when it matters most.
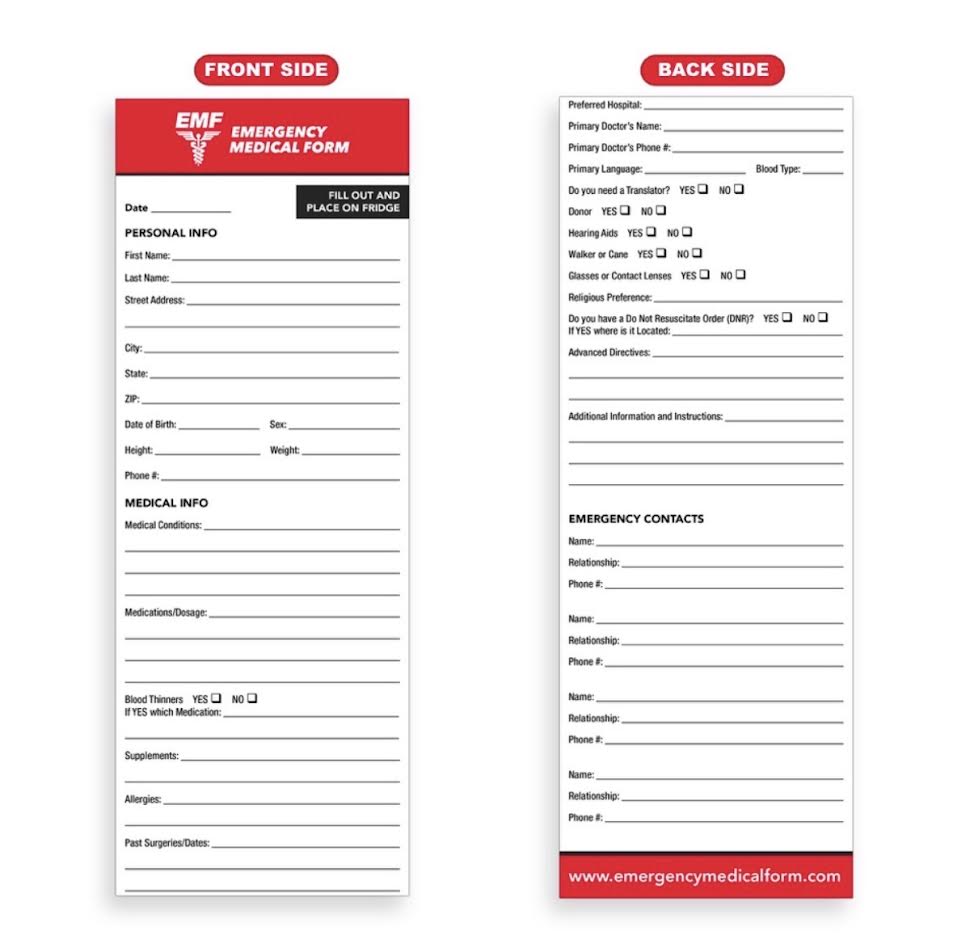
Fill out your form
Complete your emergency medical information — conditions, medications, allergies, and emergency contacts.
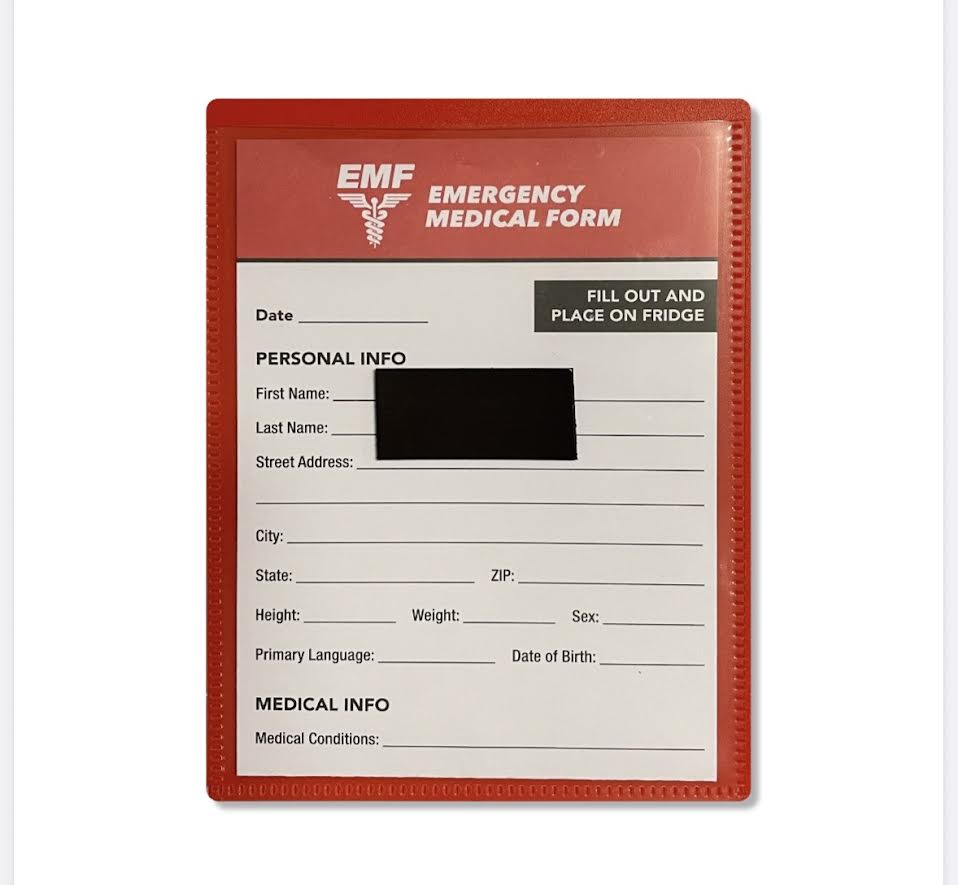
Place it in the packet
Slide your completed form into the magnetic emergency packet we provide.
Put it on your refrigerator
Stick the magnetic packet on your fridge where it's easy to find in an emergency.
What You'll Receive
A clear, easy-to-read emergency medical form and a durable magnetic packet — completely free and mailed right to your door.
Help Us Keep This Free
Optional donations help cover product and shipping costs so we can continue providing free emergency medical forms.
Thank you for your support.
Every contribution helps us mail more free emergency medical forms and magnetic packets to families.
Donate100% optional — your free form and packet are yours regardless.
Enter Your Information Below
Your emergency medical form and magnetic packet are provided at no cost — we'll mail them directly to the address you enter below.
This packet helps families prepare.
The Emergency Medical Form was made possible by Financial Health — because being ready for an emergency is part of protecting the people you love.
Have questions about life insurance, wills & trusts, medical directives, or power of attorney? Reach out for a complimentary Financial Health Checkup.
Jeff Schemansky
Financial Health — Firefighter / Paramedic
Call or Text — (586) 371-2312
Financial Health
Helping young families become more financially organized so they can enjoy life more.
Protect. Build. Grow. — Protecting What Matters Most.
Free Consultation — (586) 371-2312